
Many a truth in jest…
Many a truth in jest…
Phil Hammond’s http://www.drphilhammond.com/ inside view is that they are running the NHS at a level which is causing more and more people to turn to private providers to deliver anything above the absolute minimum. Once people come to accept that it’s more effective to go private than to demand that the NHS gives you full-coverage treatment they will have won. More healthcare will be delivered privately and the time will surely come when the NHS will be retired. He banged home the point that the NHS is funded at a level well below the EU average. The budget is about £2k per person per year. Try asking US healthcare providers whether they’ll give you full coverage for that, and be prepared to be laughed at.
There are some who argue on ideological grounds that the NHS can’t cope with the demands of our society as its age profile changes. They’re a small minority though and everyone else recognises them as simply wrong. The alternative approach, of gradually forcing us into the hands of the private providers on pragmatic grounds, is much more subtle and looks frighteningly likely to succeed.
VB
Minority? Most people in the NHS I know from those on the front line, the commissioners and up to the Department of Health think that the current model of delivery is flawed and can’t cope with inflation of costs and an ageing population.
The major problem is right or wrong they haven’t explained what they think the answer is, or funded the proposed changes properly. So all the public is going to see is access going down, a service under strain and the health system trying to shut beds by stealth which looks crazy when hospitals are under such pressure.
All of which doesn’t discount in any way the idea that the government may be trying to squeeze access and force people into private care. The flaw with this is that private providers only cherry pick the profitable procedures like orthopaedics for example. The vast majority of care is bog standard general medicine and largely loses money which is subsidised in the NHS by surgical income.
If that’s the governments plan then quite apart from the ethics of it, it just plain won’t work.
We might be talking at cross-purposes here. The hard-liners I had in mind are the ones who believe that a health service which is open to all (all UK nationals*, that is), free at the point of use and managed and staffed directly by the state without the diversion of funds into the pockets of private sector shareholders, cannot deliver the care that people need. I think that that ‘model of delivery’ would work better than any other if only it was funded properly. They disagree.
If by ‘model of delivery’ however we mean the current arrangement
which front line practitioners have to drag around like the chains on Marley’s ghost then I agree. If we burden any system sufficiently at the same time as resourcing it insufficiently then it will fail under the strain.
VB
*I’m not sure if nationals is the right word - it might be citizens or some such. You know what I mean though - those who are legitimately entitled.
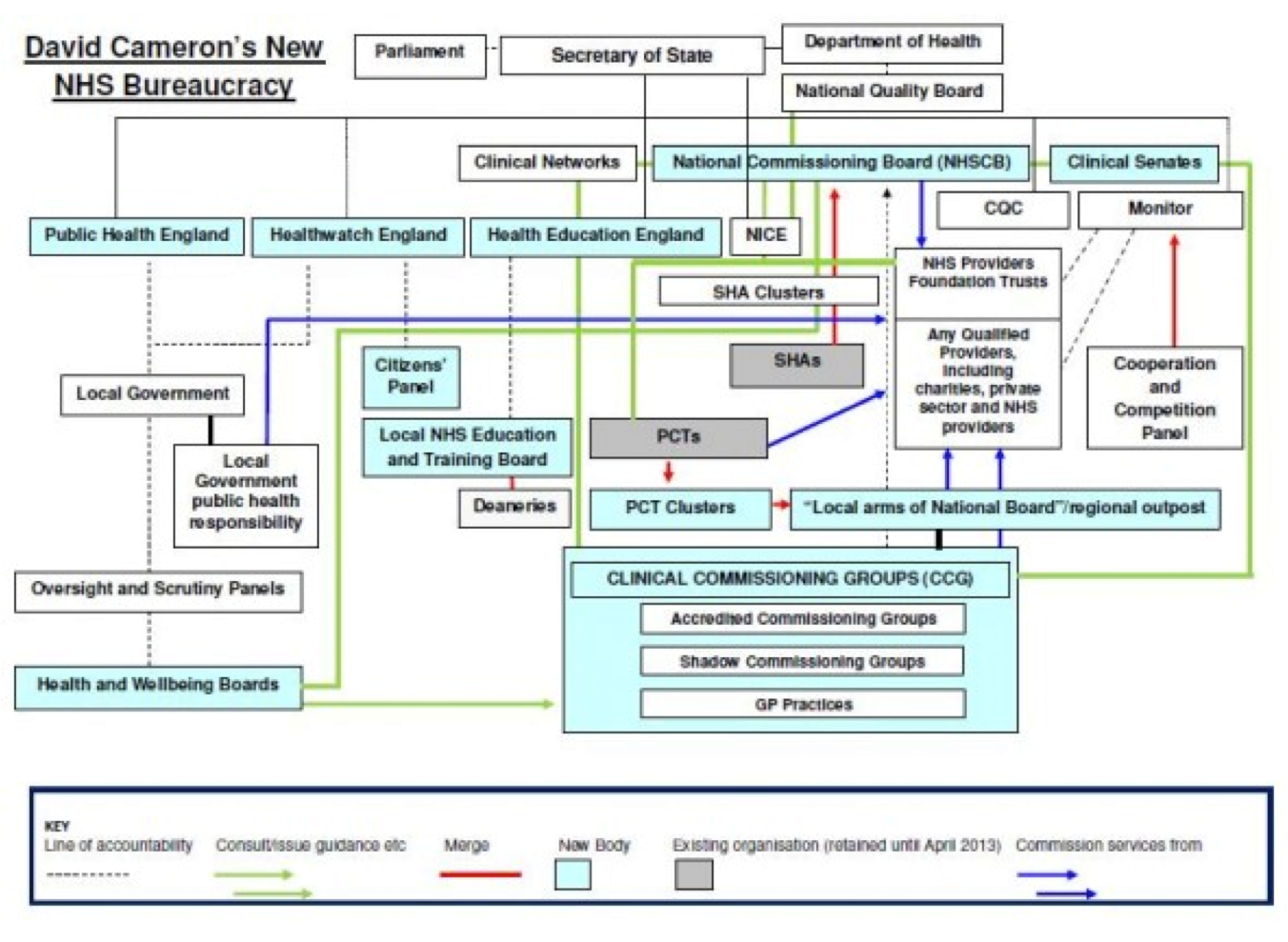
Yes we are probably at cross purposes. I would describe the diagram above as a high picture of governance (the NHS bloody loves governance and spends (wastes) inordinate amounts of time on it (I exclude clinical governance which is obviously very important).
I think you’re describing the funding model. To a point I think the funding matters only once the delivery model is sorted out. The delivery model at the moment is an out dated consultant/ acute hospital centric one, in which it assumes that everyone’s care and treatment needs to be delivered or supervised by the most specialised and expensive people in the most expensive facilities. It is disproportionately bed based (which I like to call horizontal queuing) and delivers pretty poor outcomes if you’re unlucky to be over 75 (ie the vast majority of acute bed day users). Its also completely unequipped to deal with the growing cost inflation of new treatments and an ageing population who will live longer with more long term health conditions.
Moving increasing elements of this from public to private sector will not change this underlying problem. It is the equivalent of trying to change the colour of the ocean by standing on a pier and pissing into the sea. I think you’re right though, some very limited people whose only grasp on any problem is their own flawed ideology/ dogma, will entirely fail to see this and keep repeating the same thing about markets, competition and private sector involvement.
OK, thanks, you have got me onto the right page and I agree with the above. I’ve experienced all of that first hand with
a) my stepfather, stuck for 6 months (!) in a geriatric bed with worsening vascular dementia when what he really needed and wanted (insofar as he could want anything) was an attentive and communal care home. How it took SIX MONTHS to find that for him I am still at a loss to explain,
b) my mother who lived for 18 months with terminal cancer in the care of a gifted and sensitive but hugely overworked consultant, a GP who meant the very best but who struggled to keep up with the speed at which both the disease and the consultant’s treatment of it were progressing and a huge raft of other people (district nurses, occupational health (?), social services, MacMillan, Age Concern, Maggie’s centre, her pharmacist, the hospice etc etc) many of whom seemed well meaning but a bit too keen on information gathering, assessment, advice, liaison, ‘support’ etc rather than the actual business of giving her the daily injections she needed or helping her to the loo when her mobility got worse (“an ounce of help is worth a pound of pity”). This did improve somewhat when a home care team was found for her but they were away from her for long enough each day that they couldn’t be relied upon to handle anything which cropped up urgently.
This second part of the picture - the GP and the vast horde of others - is, IMHO, the bit which needs sorting out first. At the very least there are way, way, WAY too many of them. It was tough enough for my sister, my brother and me to manage them all, and we were three fit and reasonably competent people. How a sick person, or a struggling old person is meant to cope I have no idea. If I could change one thing it would be to put a single advocate, acting for the patient and with real executive authority between the patient and the horde.
Speaking personally, I do like being under the care of a consultant though. Case in point: many diabetics are looked after through their GPs, often by a nurse who has had diabetic training. That’s not my situation though. My only contact with my GP surgery regarding my diabetes is to have blood taken there a few weeks before my clinic appointment with the specialists at the hospital. The GP phlebotomist keeps asking me whether the blood, which is going to analysed for HbA1c - a measure of the amount of glucose bonded to my haemoglobin - needs to be taken with me fasting. She thinks it does need to, despite this being a real nuisance for me. I finally got round to asking my consultant whether I needed to be fasting. “No” he said “the haemoglobin attaches glucose slowly and continuously over the red blood cells’ few month lifetime and whether you happen to have eaten or not in the few hours before it’s taken is immaterial. Furthermore, if you get any more grief tell them that I’ve told you this and that I’m the person who invented the HbA1c test !”. When your long-term health is in the balance it is comforting to be in the hands of someone who treats your condition, and only your condition and who is not just keeping up with the very latest developments but is actually making them.
VB
I have been unyellowed by a particularly clever surgeon who has yanked out a length of my innards. Therefore, you may, with all due respect, feck right off.
![]()
Bah, Willy Wonka would have sorted you out much quicker in the dejuicing room.

Blue? Meh! Dejuicing is for pussies. I’m more of a fan of partial disembowelling to deal with the yellow. We’ll need a sliver off the liver ( ) next year too, so much more fun than yer Oompah Lumpah assisted squeezery.
) next year too, so much more fun than yer Oompah Lumpah assisted squeezery.

A length? Unless you’re a member of the multiple lengths club you is, like, a total fanny ![]()
This was my second re-section in 7 years. I iz not da fanny thusly
OK. I’m struggling to compete here.
Uhh, the ominously named Mr Brown also stitched up my bladder? Nah, doesn’t really cut the mustard, does it.
But the liver was dry
Could you set the whole of your condition to American Pie?
Anyway, it’s not the length that matters, it is the quality of the yanking. 
Bladders are a shocker. I’m terrified of catheters so anything more complex water-works related is just  as far as I’m concerned.
as far as I’m concerned.
No, that would be hideous. I guess mellow yellow might have a chance though.
This thread is disturbingly like the scene in Jaws where Quint and Hooper compare shark bite scars, while Brody is embarrassed by his mere appendectory scar. I am Chief Brody here, with only some tiny polyps having been removed from my shit pipe.
When do we start singing “Spanish Ladies”?
Edit: Actually, it was a medley with “Show me the way to go home”
![]() fixt for accuracy
fixt for accuracy
Perhaps it’s not a bad thing that Trump will immolate us all.
